
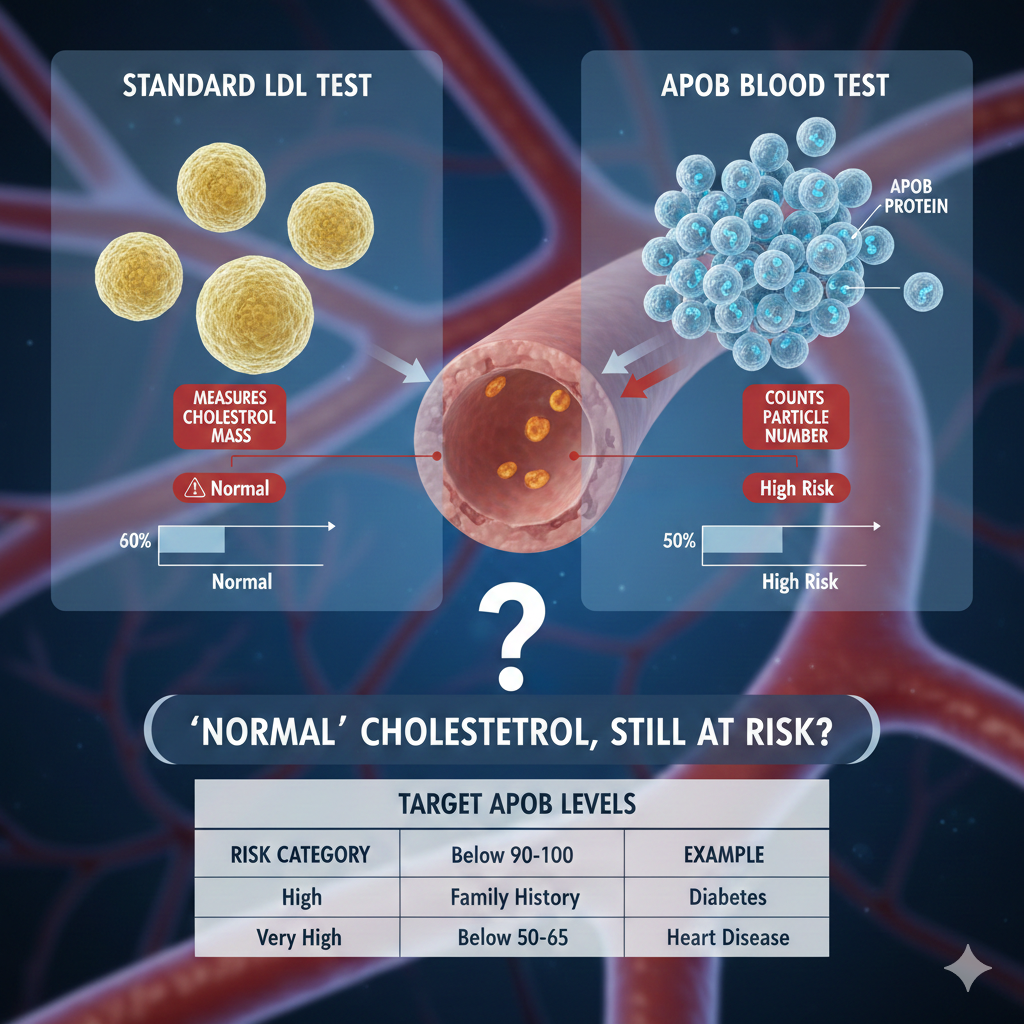
Could “Normal” Cholesterol Still Put You at Risk?
Your cholesterol numbers might look perfectly fine on paper — yet hidden artery-clogging particles could still be quietly raising your risk of a heart attack. The ApoB blood test may reveal what a standard lipid profile misses.
What Is the ApoB Blood Test?
ApoB (Apolipoprotein B) is a blood test that measures the number of harmful cholesterol particles circulating in your blood. Every atherogenic (artery-clogging) lipoprotein particle — including LDL, VLDL, IDL, and Lp(a) — carries exactly one ApoB protein. By counting ApoB proteins, the test tells your doctor how many of these particles are present, not merely how much cholesterol they contain.
How Is ApoB Different from Standard LDL Testing?
A traditional LDL test measures the amount of cholesterol packed inside LDL particles. ApoB measures how many particles exist in the first place. This distinction matters because you can have a normal LDL cholesterol reading while still carrying a dangerously high number of particles. Since each particle carries one ApoB protein, ApoB provides a more direct and precise estimate of cardiovascular risk than LDL alone — particularly in people with high triglycerides, insulin resistance, or metabolic syndrome.
Why Is Particle Count So Important?
Heart disease develops when cholesterol particles penetrate and accumulate inside artery walls, forming plaques. The number of particles — not just their cholesterol content — determines how aggressively this process occurs. ApoB directly reflects total atherogenic particle count, plaque-forming potential, and residual risk in patients already receiving treatment. For these reasons, many preventive cardiologists now consider ApoB a superior risk stratification tool.
Who Should Consider Getting an ApoB Test?
A physician may recommend an ApoB test for individuals who have a family history of early heart disease, diabetes, or metabolic syndrome, or who are overweight or have high triglycerides. It is also valuable for people whose standard LDL results do not fully explain their apparent cardiovascular risk, and for those already on statins who need more precise monitoring of residual risk.
How Is the Test Performed?
A small blood sample is drawn from a vein in the arm. Fasting is generally not required when ApoB is tested in isolation. If it is ordered alongside a full lipid panel, your doctor may ask you to fast for 10 to 14 hours beforehand. Always follow your physician’s specific instructions.
Understanding Your Results
Higher ApoB levels indicate a greater number of artery-clogging particles and a correspondingly higher risk of heart attack and stroke. Lower levels suggest better cardiovascular protection. General target thresholds — which vary according to individual risk — are outlined below. Your doctor will always interpret results within the context of your overall health profile.
Target ApoB Levels by Risk Category
The following targets reflect current guidance from leading cardiovascular societies. Individual recommendations may differ based on your clinical situation.
Moderate risk: below 90–100 mg/dL
High risk (for example, diabetes or known heart disease): below 65–80 mg/dL
Very high risk or secondary prevention: below 50–65 mg/dL
How Is ApoB Used in Treatment?
The test helps physicians estimate cardiovascular risk more accurately, determine whether treatment is warranted, and monitor how effectively medications such as statins, ezetimibe, PCSK9 inhibitors, and bempedoic acid are lowering particle burden. Because LDL levels can appear well controlled while particle counts remain elevated, ApoB is especially useful for identifying residual risk in patients already on therapy.
Can ApoB Levels Be Reduced?
Yes. Both lifestyle changes and medications can meaningfully lower ApoB.
On the lifestyle side, weight reduction, regular physical activity, lower intake of refined carbohydrates, and reduced saturated fat consumption have all been shown to decrease particle counts.
On the medication side, statins, ezetimibe, PCSK9 inhibitors, and bempedoic acid are the most commonly used agents. Lowering ApoB reduces cardiovascular risk regardless of which approach is used.
Is ApoB Better Than Non-HDL Cholesterol?
Both measures are clinically useful. Non-HDL cholesterol estimates the total cholesterol content across all atherogenic particles. ApoB goes a step further by directly counting those particles, which can provide more precise risk assessment — particularly in patients with elevated triglycerides or metabolic syndrome. In most situations, ApoB offers the more granular picture.
Common Questions
Does a high ApoB guarantee a heart attack? No. ApoB is a risk marker, not a diagnosis. Risk assessment is always multifactorial and must account for blood pressure, blood sugar, family history, smoking status, and imaging findings where appropriate.
Is ApoB included in a routine cholesterol test? No. It must be ordered separately, though more laboratories now include it as part of advanced lipid panels.
Should everyone get an ApoB test? Not necessarily. For low-risk individuals with normal lipid profiles and no significant risk factors, a standard lipid panel may be sufficient. ApoB testing is most valuable in intermediate- to high-risk patients, those with diabetes or metabolic syndrome, and anyone with unexplained cardiovascular risk. Discuss with your physician whether it is appropriate for you.
Recent ApoB Research (2025-Early 2026): What We Know
Aortic Stenosis & ApoB: A January 2026 JACC: Advances study confirms that elevated ApoB levels are associated with worse outcomes in patients with aortic stenosis, supporting ApoB’s prognostic role beyond traditional lipid markers.
ApoB/ApoA-I Ratio: A large December 2025 case-control study found the ApoB/ApoA-I ratio to be the strongest independent lipid predictor of coronary heart disease (CHD), acute myocardial infarction (AMI), multivessel disease, and need for PCI — with predictive strength especially high in males, older adults, and hypertensive patients, and attenuated among diabetics.
Guidelines (2025–Early 2026): No major global guideline revisions have fundamentally altered ApoB’s established role. ESC/EAS, ACC/AHA, and expert bodies still position ApoB as an informative marker — especially in selected high-risk patients, metabolic syndrome, or where LDL-C does not fully capture risk. Expert lipid societies continue to emphasize ApoB’s value in tailored risk assessment and treatment monitoring.
What the Major Clinical Guidelines Say
The table below summarizes how leading cardiovascular organizations position ApoB in clinical practice.
Organization — ACC / AHA (2018 Guideline)
Position: Recognized as a risk-enhancing factor
When recommended: Elevated triglycerides (200 mg/dL or above), intermediate-risk patients
Key threshold: ApoB at or above 130 mg/dL is considered a risk-enhancing level
Organization — ACC Expert Consensus (2022)
Position: Useful for residual risk assessment and therapy monitoring
When recommended: Patients on statins, or those with discordant LDL and triglyceride results
Key threshold: No universal target; used to guide intensification of therapy
Organization — ESC / EAS (2019 Guideline)
Position: An alternative and sometimes preferred risk marker
When recommended: Diabetes, metabolic syndrome, obesity, high triglycerides
Key thresholds: Below 100 mg/dL for moderate risk; below 80 mg/dL for high risk; below 65 mg/dL for very high risk
Organization — Canadian Cardiovascular Society (2021 Guideline)
Position: Recommended as a primary treatment target
When recommended: High-risk and secondary prevention patients
Key threshold: Below 80 mg/dL for high-risk patients
ApoB/ApoA-I Ratio: A Simple Guide for Patients
What Is the ApoB/ApoA-I Ratio?
The ApoB/ApoA-I ratio is a blood test that helps measure your risk of heart disease.
It compares:
ApoB – a marker of “bad” cholesterol particles that can clog your arteries
ApoA-I – a marker of “good” cholesterol particles that help remove cholesterol from your arteries
Think of it as a balance test:
ApoB = particles that can cause plaque buildup
ApoA-I = particles that help clean up cholesterol
The ratio shows which side is winning.
Why Does This Ratio Matter?
Heart disease develops when too many harmful cholesterol particles enter artery walls and form plaque.
If your:
ApoB is high → more plaque-forming particles
ApoA-I is low → less protection
A higher ratio means more risk.
A lower ratio means better protection.
Why Not Just Check LDL (“Bad” Cholesterol)?
Traditional cholesterol tests measure how much cholesterol is in your blood.
The ApoB/ApoA-I ratio looks deeper:
It counts the number of harmful particles (not just the cholesterol amount)
It compares them to protective particles
It may detect hidden risk even when LDL looks “normal”
This is especially helpful if you have:
• Diabetes
• High triglycerides
• Metabolic syndrome
• Family history of heart disease
• “Normal” cholesterol but ongoing concern
What Is a Good ApoB/ApoA-I Ratio?
There are no strict universal cutoffs, but generally:
Below 0.50–0.60 → Lower risk
Around 0.70–0.90 → Moderate risk
Above 0.90 (men) or 0.80 (women) → Higher risk
Lower is better.
Your doctor will interpret your result along with:
• Blood pressure
• Blood sugar
• Family history
• Other cholesterol numbers
• Imaging tests (if needed)
Can You Improve the Ratio?
Yes. The main goal is to lower ApoB, because ApoB particles cause artery damage.
Ways to improve it:
Lifestyle:
• Maintain healthy weight
• Exercise regularly
• Reduce refined carbohydrates
• Eat less saturated fat
• Stop smoking
Medications (if needed):
• Statins
• Ezetimibe
• PCSK9 inhibitors
• Bempedoic acid
Lowering ApoB reduces heart risk.
Raising ApoA-I through lifestyle (exercise, healthy diet) helps — but lowering ApoB is more important.
Is This Test Routine?
No. It is not included in most standard cholesterol panels. Your doctor must order it separately.
It may be useful if:
Your risk seems unclear
You are already on cholesterol medication
Your LDL looks normal but concern remains
Important to Know
This test does not diagnose heart disease by itself.
It is one piece of your overall risk picture.
Risk is continuous — there is no single “magic number.”
Always discuss results with your healthcare provider.
In Simple Terms
The ApoB/ApoA-I ratio shows the battle between harmful and protective cholesterol particles in your blood.
If harmful particles outnumber protective ones, your risk rises.
If protective forces are stronger, your arteries are better defended.
If you have risk factors or borderline cholesterol, this test can provide clearer insight into your true heart risk.
Quick FAQ: ApoB/ApoA-I Ratio
1. Is this test better than a regular cholesterol test?
It’s not a replacement — it’s an upgrade in certain situations.
A regular lipid panel measures cholesterol amounts.
The ApoB/ApoA-I ratio looks at the balance between harmful and protective particles, which can sometimes reveal hidden risk.
2. If my LDL is normal, do I still need this test?
Maybe. Some people have normal LDL but still carry a high number of harmful particles.
If you have diabetes, high triglycerides, family history, or unexplained risk, your doctor may consider this test.
3. Does a high ratio mean I will definitely have a heart attack?
No. It means your risk is higher — not that an event will definitely happen.
Heart disease depends on many factors, including blood pressure, smoking, blood sugar, genetics, and lifestyle.
4. Can I lower my ApoB/ApoA-I ratio naturally?
Yes. Healthy habits can improve it:
• Regular exercise
• Weight control
• Balanced diet with fewer refined carbs and saturated fats
• Avoiding tobacco
If needed, medications can further lower ApoB and reduce risk.
5. Is this test routinely done?
No. It is not included in most standard cholesterol panels.
It must usually be ordered separately, often by a cardiologist or lipid specialist.
6. What matters more — ApoB or the ratio?
Most experts agree that lowering ApoB (harmful particle number) is the main goal.
The ratio provides helpful context but treatment usually focuses on reducing ApoB.
Authoritative Resources for Further Reading
Full guideline in the Journal of the American College of Cardiology:
https://www.jacc.org/doi/10.1016/j.jacc.2018.11.003
ESC / EAS 2019 Dyslipidaemia Guidelines:
Canadian Cardiovascular Society 2021 Dyslipidemia Guideline:
National Lipid Association:
These recommendations reflect guidance from the ACC/AHA, the European Society of Cardiology, and the Canadian Cardiovascular Society, representing current global standards in preventive cardiology. Individual clinical decisions should always be made in consultation with a qualified physician.
Medical & Educational Disclaimer
This content is provided for general educational purposes only and is not intended as medical advice, diagnosis, or treatment. Cardiovascular risk assessment is complex and individualised. Laboratory values such as ApoB or the ApoB/ApoA-I ratio should be interpreted by a licensed healthcare provider within the context of your overall health profile. Never delay or disregard professional medical advice because of information you have read here.
Explore more at the Rise & Inspire archive | Motivational Blogs
© 2025 Rise & Inspire. Follow our journey of reflection, renewal, and relevance.
Website: Home | Blog | About Us | Contact| Resources
Word Count:2089